
Non-Alcoholic Fatty Liver Disease (NAFLD) has emerged as a leading cause of chronic liver disease, affecting a significant portion of the global population. Defined as the accumulation of excess fat in the liver not related to alcohol consumption, NAFLD is closely linked to metabolic syndrome - a cluster of conditions that increase the risk of heart disease, stroke, and diabetes. Any condition that contributes to metabolic syndrome can potentially contribute to the development of NAFLD but underlying endocrine disorders may also promote the development and progression of this common liver disorder. Additionally, exposure to environmental and chemical toxins may also promote the development of NAFLD. In the following article, we will take a closer look at some of the contributing factors and specifically examine endocrine-related and secondary causes of NAFLD.
Prevalence and Disease Progression
In the United States, one-third of the population has NAFLD and 2-5% have progressed to non-alcoholic steatohepatitis (NASH). NASH involves inflammatory processes in the presence of fatty infiltration (NAFLD) and can ultimately progress to liver fibrosis, cirrhosis, and liver cancer. In 20-25% of NAFLD cases, steatosis (fatty infiltration) will evolve to NASH and 20% of these patients will develop cirrhosis. The progression to NASH often occurs in the presence of diabetes, insulin resistance, and other preexisting conditions associated with metabolic issues (1).
Diagnosis of NAFLD
The definitive diagnosis of NAFLD is via liver biopsy showing lipid content in at least 5% of hepatocytes (liver cells). Only biopsy can assess inflammation and fibrosis, but diagnosis can be inaccurate due to sampling variability (1).
Less invasive diagnostic methods do exist using various types of imaging techniques that can measure liver fat content. Proton magnetic resonance spectroscopy is the most accurate, but ultrasound is the most common diagnostic method. The drawback is that ultrasound can only detect liver fat content when it exceeds 35% (1).
Elevation in liver enzymes can be a clue to liver fat accumulation, but these measurements are neither specific nor sensitive. Up to 70% of those with NAFLD will have normal liver enzymes. Regardless, a diagnosis of NAFLD should be considered if there are elevated liver enzymes and one metabolic risk factor such as insulin resistance, high cholesterol, hypertension, atherosclerosis, and obesity (1).
Development and Progression of NAFLD
The progression of liver injury in NAFLD is thought to result from the “two hit” hypothesis involving insulin resistance and adipokine production. The “first hit” involves the accumulation of triglycerides (TG) and free fatty acids (FFA) in hepatocytes secondary to insulin resistance. Once fatty infiltration is established, progression to steatohepatitis involves the “second hit” which consists of inflammation, mitochondrial dysfunction, and enhanced oxidative stress resulting from reactive oxygen species (ROS), lipid oxidation, and ongoing production of adipokines (1).
Adipokines are cytokines (cell-signaling molecules) released by adipose tissue that mediate inflammation and contribute to metabolic issues. The combination of insulin resistance and adipokine production can result in oxidative stress and cell death (apoptosis). Ultimately, this can lead to hepatocyte damage and fibrosis. Other factors that can impact liver injury involve gut bacteria that further promote inflammation (1).
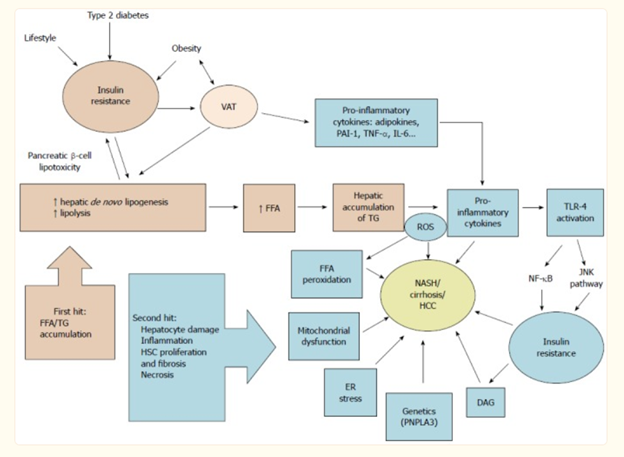

Fig 1. Schematic summary of NAFLD pathophysiology according to the "two-hit hypothesis".
Main Causes of NAFLD
The main physiological mechanism associated with the development of NAFLD is insulin resistance which often leads to obesity, metabolic syndrome, type II diabetes, and dyslipidemia. An unhealthy lifestyle is considered a modifiable risk factor for NAFLD. The key factors that contribute to metabolic dysfunction that may promote the development of NAFLD are common to many diseases.
High-carbohydrate/high-sugar diet - Excessive consumption of simple carbohydrates and high-sugar foods often lead to insulin resistance and the accumulation of visceral adipose tissue (VAT) that becomes dysfunctional and produces an excess of pro-inflammatory cytokines leading to excessive systemic inflammation thus worsening insulin resistance (2). According to research out of UC, San Diego, fructose in particular, can drive fat accumulation in the liver and increase gut permeability leading to an increase in circulating endotoxins. The inflammatory process induced by endotoxins enhances fatty deposition in the liver and progressive inflammation (3).
Sedentary lifestyle – Reduced physical activity contributes to weight gain and metabolic risk whereas, regular exercise increases insulin sensitivity, helps to manage weight, and reduces the risk for conditions associated with metabolic syndrome. Physical activity and regular exercise are key regulators of metabolism and have a measurable impact on several drivers of metabolic disease. Ultimately, along with dietary changes, exercise can help manage weight and moderate stress (4).
Insufficient sleep – Reduced quality and quantity of sleep can disrupt hormonal balance, leading to increased appetite and weight gain, further exacerbating metabolic issues. Researchers out of China analyzed self-reported sleep behaviors from 5,011 Chinese adults with fatty liver disease and found late bedtime, snoring, and daytime napping for over 30 minutes were significantly associated with an increased risk of fatty liver disease. Most participants qualified as having measurable markers associated with metabolic issues. The study revealed that even a moderate improvement in sleep quality led to a 29% reduction in fatty liver disease risk (5).
Ongoing stress – Though stress is a part of life, ongoing stress with no end in sight, can lead to chronically elevated cortisol and catecholamines that may promote weight gain and the accumulation of VAT. The association of perceived stress with cardiovascular and metabolic abnormalities has been well-documented. Stress can be a component of nearly every disease process because of fundamental endocrine, metabolic, and cardiovascular dysregulation that occurs in the presence of ongoing stress (6).
Endocrine-Related Disorders and NAFLD
NAFLD and metabolic syndrome are the most common causes of NASH, but NAFLD itself may be linked with other endocrine disorders. (1). These common endocrine disorders can significantly impact metabolic health, often contributing to the development of metabolic syndrome. Hormonal imbalances can alter insulin sensitivity, fat metabolism, and have effects on appetite regulation.
Hypothyroidism – Thyroid hormones are integral to hepatic lipid metabolism. Thyroid hormones promote lipolysis within the liver thus modifying hepatic fat accumulation. Hypothyroidism has been associated with disorders of glucose and insulin metabolism and high cholesterol, which are both associated with metabolic syndrome. Though there is no cause/effect relationship between hypothyroidism and NAFLD, hypothyroidism may be an independent risk factor for NAFLD as some studies report a prevalence of hypothyroidism of 15.2–36.3% among patients with NAFLD/NASH (1).
Subclinical and overt hypothyroidism may cause secondary NAFLD but may also worsen primary NAFLD. Interestingly, thyroid hormone receptor agonists are currently being evaluated for the treatment of NASH and have proven effective in reducing hepatic fat accumulation after 12 and 36 weeks of treatment in a phase II trial (7).
PCOS – Insulin resistance occurs in approximately 50% of women with PCOS. The prevalence of NAFLD in PCOS women occurs somewhere between 15% and 55%. In a study that compared the prevalence of NAFLD amongst lean and obese women with PCOS, 39% of the lean women had NAFLD. In addition to the known effects of insulin resistance, hyperandrogenism likely plays a key role in the development of NAFLD as it is associated with down-regulation of the LDL-receptor. This prolongs the half-life of VLDL and LDL, inducing the accumulation of fat in the liver (8).
In premenopausal women, hyperandrogenism is associated with increased visceral fat and insulin resistance, and an increase in free testosterone shows a greater association with NAFLD. Elevated sex hormone binding globulin (SHBG) can also be associated with an increased risk of developing NAFLD and might be considered a good surrogate marker for the severity of NAFLD if metabolic issues are not present (8). Additionally, women with hyperandrogenism tend to have higher levels of liver enzymes, particularly ALT (1).
Growth Hormone Deficiency – Growth hormone (GH) has several important functions in adults, including maintenance of lean body and bone mass, promoting lipolysis thus limiting visceral adiposity, and regulating carbohydrate metabolism, cardiovascular function, aerobic exercise capacity, and cognitive function. GH deficiency can be the result of hypopituitarism that may be caused by tumors, brain injuries, infections, genetics, or medications. GH deficiency is also associated with normal aging where production peaks in puberty and declines by 15% every decade starting in the third decade of life. GH deficiency may be an underlying factor in secondary NAFLD. In a Japanese study of patients with GH deficiency, 77% had NAFLD as compared to age-, sex-, and BMI-matched controls (10).
Age-Related Hormone Loss – Aging and sex hormone loss are also risk factors for the development of NAFLD as there is a bidirectional relationship between metabolic issues and loss of sex hormones as both men and women age. In both males and females, insulin resistance and metabolic syndrome are associated with an increase in visceral adipose tissue (VAT) that becomes dysfunctional and produces an excess of adipokines and pro-inflammatory cytokines leading to excessive systemic inflammation. Adipokines are cytokines produced by adipose tissue and are involved in adipose homeostasis and lipid metabolism. Leptin, ghrelin, and adiponectin are adipokines that decrease insulin resistance, but their output becomes dysfunctional in the presence of excess adipose tissue and metabolic disorders (2).
Men tend to have a higher rate of NAFLD than women, but this gender association becomes less pronounced as women enter menopause. Declining androgens in males and declining estrogen in women are associated with features of metabolic syndrome in both sexes as they age. Sex hormones have effects on energy homeostasis with testosterone directing adipose tissue physiology via androgen receptors by preventing adipose accumulation and maintaining lean body mass in men. Studies have shown an association between low testosterone and increased sonographic evidence of hepatic fat accumulation in men (2).
Hypercortisolism – As mentioned above when discussing stress as a contributing factor to the development of NAFLD, high levels of cortisol can impair insulin sensitivity leading to insulin resistance. The extreme effects of hypercortisolism can be demonstrated in Cushing’s syndrome which is a disease of high cortisol caused by over-exposure to corticosteroids or pituitary or adrenal tumors that ultimately increase output of cortisol from the adrenal glands. Cushing syndrome is associated with the development of insulin resistance, type II diabetes, dyslipidemia, hypertension, visceral obesity, and NAFLD (1). Hypercortisolism in response to ongoing stress combined with other contributing factors that promote metabolic issues may result in a similar presentation.
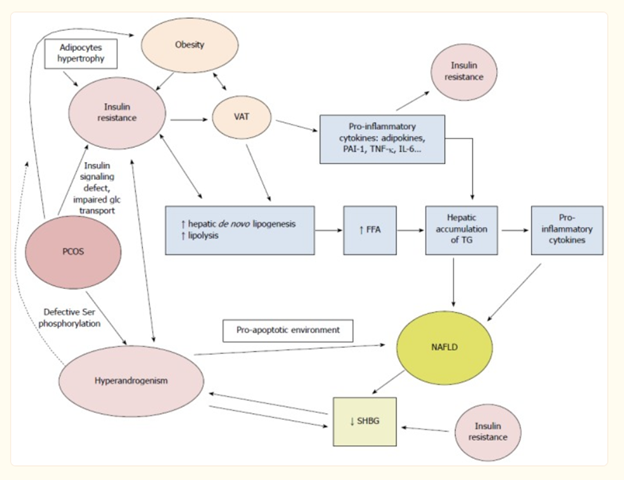
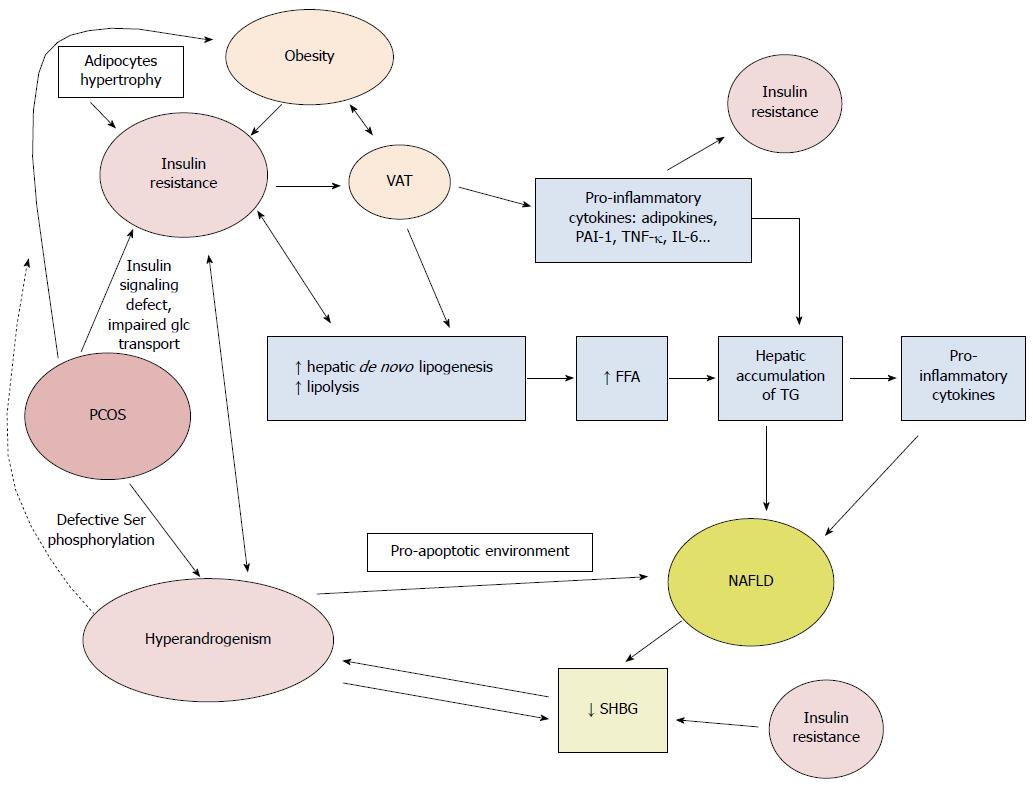

Fig. 2: Pathophysiological mechanisms linking polycystic ovary syndrome and NAFLD.
HRT and NAFLD
Some studies suggest that estrogen may play a regulatory role in the development of NAFLD. Estrogen exerts anti-steatotic effects thus preventing fat accumulation in hepatocytes. Estrogen also has an anti-inflammatory effect in the Kupffer cells which function as macrophages and are key to healthy liver function (11).
Hormone replacement therapy (HRT) can reduce the development of NAFLD, but route of delivery is determinate of its benefits. In 2024, Kim et al conducted a 12-month retrospective cohort study evaluating the benefits of transdermal vs. oral estrogen in reducing the development or progression of NAFLD. The study included 368 menopausal women of similar health status. Seventy-five women received transdermal estradiol and 293 received oral estrogen as either estradiol or conjugated equine estrogens. Women with a uterus received either oral micronized progesterone or a synthetic progestin. All were evaluated for NAFLD via ultrasonography, liver function tests, fasting glucose and insulin, HgA1c, and a lipid panel. Insulin resistance was evaluated using the homeostasis model assessment of insulin resistance (HOMA-IR) calculation (11).
Prior to treatment, 24% of the women in the transdermal group were positive for NAFLD. After 12 months on transdermal estradiol, only 17.3% were positive for NAFLD. In the group of women on oral estrogen, 25.3% were positive for NAFLD prior to hormone treatment, but this increased to 29.4% after 12 months of oral estrogen (11).
Secondary Causes/Contributors to NAFLD and NASH
Not all subjects with NAFLD experience obesity, insulin resistance, diabetes, and endocrine disorders, so there are other factors that can contribute to this pathologic spectrum of liver diseases. As part of the “two-hit” hypothesis of the development of NAFLD and NASH, there is the potential contribution of occupational and environmental chemicals (12).
Toxicant associated steatohepatitis (TASH) describes a liver condition in which fatty infiltration occurs associated with excessive exposure to various chemicals including volatile organic chemicals (VOCs), persistent organic pollutants (POPs), metals, particulate matter, and pesticides. Many of these chemicals can be classified as endocrine disruption chemicals (EDCs), metabolism disrupting chemicals (MDCs), and signaling disrupting chemicals (SDCs). EDCs interfere with aspects of hormone function and MDCs promote metabolic changes that can result in obesity and type II diabetes. Many of these chemicals are known to be hepatotoxic and are cleared from the body through liver detoxification pathways (12).
Gut microbiota and NAFLD
Gut microbiota plays an important role in human metabolism and the metabolites of gut flora have effects on organ systems and tissues throughout the body. The liver is exposed to a high concentration of bacterial metabolites as it is closely linked to the intestines through the gut-liver axis and is the first organ to receive blood from the intestines via the portal system. Pathogenic bacteria along with a leaky gut can trigger a pathological reaction in the liver as well as contributing to metabolic disorders (8).
Enhanced intestinal permeability coupled with an abundance of LPS-producing gram-negative bacteria can lead to liver inflammation by triggering toll-like receptor (TLR) signaling pathways. TLRs play a central role initiating an immune response in the presence of microbial antigens. Increased levels of LPS and the resulting cytokines can promote the proliferation and deposition of intrahepatic fibrous connective tissue that results in cirrhosis. The presence of LPS in the liver also results in intrahepatic resistance to blood flow which can lead to portal hypertension that can further damage the liver (9).
Treatment of NAFLD
NAFLD is one of the top reasons for liver transplants. It’s hard to believe that poor diet and lifestyle can potentially lead to the need to replace a major organ. Even though the liver is a workhorse with the capacity to regenerate itself, it can’t hold up to the ongoing effects of metabolic disease, fatty infiltration, and inflammation. On a positive note, diet and lifestyle modifications have great potential in the primary prevention of NAFLD. Adopting a healthy lifestyle that includes maintaining a normal body mass index (BMI), eating in line with a Mediterranean diet, cutting back on sedentary behavior, and engaging in daily physical activity can lower the risk of NAFLD. In the larger picture, reducing exposure to toxins and keeping the endocrine system balanced can also have positive and lasting effects.
Randomized controlled trials demonstrate that dietary and exercise interventions for NAFLD reduce BMI, steatosis, and inflammation as determined by MRI and biopsy. The Mediterranean diet seems to be the most effective long-term approach to dietary changes with a focus on healthy fats, lots of veggies, and reduced simple carbohydrates and sugars. Consuming a variety of high-fiber veggies rich in antioxidants can not only support health in general but is also good for a healthy microbiome, which in turn, also supports a healthy liver. Most dietary and lifestyle effects far-surpass the efficacy of drugs currently being evaluated in phase III clinical trials (4).
Foods rich in choline such as fatty fish rich in omega-3s, eggs, and cruciferous vegetables can be supportive of liver function and bile production. Choline deficiency promotes the rapid progression of NAFLD to NASH. Diets deficient in choline reduce the production of phosphatidylcholine which is essential for the creation of very low-density lipoproteins (VLDLs) and results in liver fat accumulation (8). Choline is also necessary for the formation of bile and movement of fats and toxins out of the liver. Several genetic polymorphisms associated with choline metabolism have been linked to liver damage. Aside from dietary sources, choline can be supplemented directly by way of phosphatidylcholine or citicoline.
Additional nutritional supplements that are supportive of liver health include vitamin E, vitamin D, CoQ10, EGCG from green tea, prebiotics and probiotics, milk thistle, and curcumin (4, 13). Though nutritional supplements may have benefits, they are best when combined with a healthy diet and regular exercise.
The cure is in the cause
A predisposition to developing NAFLD may occur in the presence of genetic mutations that affect liver function, but the main driver of its development is diet and lifestyle in which underlying endocrine disorders, toxic exposures, and secondary causes may be contributing factors. Long-term changes in dietary and lifestyle habits can be challenging because they require education, determination, and discipline, but these changes are possible and beneficial to good health on many levels.
Definition of terms
Steatosis: fat accumulation in the liver.
Steatohepatitis: fat accumulation + inflammation.
Fibrosis: development of scar tissue in the liver to any degree.
Cirrhosis: extreme degree of scar tissue in the liver that is severe and permanent and significantly affects liver function.
VAT: Visceral Adipose Tissue
References:
1. Marino, Laura, and François R. Jornayvaz. “Endocrine Causes of Nonalcoholic Fatty Liver Disease.” World Journal of Gastroenterology : WJG, vol. 21, no. 39, Oct. 2015, pp. 11053–76. PubMed Central, https://doi.org/10.3748/wjg.v21.i39.11053.
2. Vincenzo, Angelo Di, et al. “Sex Hormones Abnormalities in Non-Alcoholic Fatty Liver Disease: Pathophysiological and Clinical Implications.” Exploration of Medicine, vol. 2, no. 4, Aug. 2021, pp. 311–23. www.explorationpub.com, https://doi.org/10.37349/emed.2021.00049.
3. Todoric J, Di Caro G, Reibe S, Henstridge DC, Green CR, Vrbanac A, Ceteci F, Conche C, McNulty R, Shalapour S, Taniguchi K, Meikle PJ, Watrous JD, Moranchel R, Najhawan M, Jain M, Liu X, Kisseleva T, Diaz-Meco MT, Moscat J, Knight R, Greten FR, Lau LF, Metallo CM, Febbraio MA, Karin M.Todoric J, et al. Nat Metab. 2020 Aug 24. doi: 10.1038/s42255-020-0261-2, https://www.nih.gov/news-events/nih-research-matters/how-high-fructose-intake-may-trigger-fatty-liver-disease
4. Hallsworth, Kate, and Leon A. Adams. “Lifestyle Modification in NAFLD/NASH: Facts and Figures.” JHEP Reports, vol. 1, no. 6, Dec. 2019, pp. 468–79. ScienceDirect, https://doi.org/10.1016/j.jhepr.2019.10.008.
5. Jialu Yang, Shiyun Luo, Rui Li, Jingmeng Ju, Zhuoyu Zhang, Jichuan Shen, Minying Sun, Jiahua Fan, Min Xia, Wei Zhu, Yan Liu, Sleep Factors in Relation to Metabolic Dysfunction-Associated Fatty Liver Disease in Middle-Aged and Elderly Chinese, The Journal of Clinical Endocrinology & Metabolism, Volume 107, Issue 10, October 2022, Pages 2874–2882, https://doi.org/10.1210/clinem/dgac428.
6. Kang, Danbee, et al. “Perceived Stress and Non-Alcoholic Fatty Liver Disease in Apparently Healthy Men and Women.” Scientific Reports, vol. 10, no. 1, Jan. 2020, p. 38. www.nature.com, https://doi.org/10.1038/s41598-019-57036-z.
7. Liebe, Roman, et al. “Diagnosis and Management of Secondary Causes of Steatohepatitis.” Journal of Hepatology, vol. 74, no. 6, June 2021, pp. 1455–71. ScienceDirect, https://doi.org/10.1016/j.jhep.2021.01.045.
8. Carrieri, Livianna, et al. “Premenopausal Syndrome and NAFLD: A New Approach Based on Gender Medicine.” Biomedicines, vol. 10, no. 5, May 2022, p. 1184. PubMed Central, https://doi.org/10.3390/biomedicines10051184.
9. Wang, Li, et al. “The Role of Gut Microbiota in Some Liver Diseases: From an Immunological Perspective.” Frontiers in Immunology, vol. 13, July 2022, p. 923599. PubMed Central, https://doi.org/10.3389/fimmu.2022.923599.
10. Garcia, Jose M., et al. “Growth Hormone in Aging.” Endotext, edited by Kenneth R. Feingold et al., MDText.com, Inc., 2000. PubMed, http://www.ncbi.nlm.nih.gov/books/NBK279163/.
11. Kim, Sung Eun, et al. “Different Effects of Menopausal Hormone Therapy on Non-Alcoholic Fatty Liver Disease Based on the Route of Estrogen Administration.” Scientific Reports, vol. 13, no. 1, Sept. 2023, p. 15461. www.nature.com, https://doi.org/10.1038/s41598-023-42788-6.
12. Wahlang, Banrida, et al. “Mechanisms of Environmental Contributions to Fatty Liver Disease.” Current Environmental Health Reports, vol. 6, no. 3, Sept. 2019, p. 80. pmc.ncbi.nlm.nih.gov, https://doi.org/10.1007/s40572-019-00232-w.
13. Baradeiya, Ahmed M., et al. “Can Nutritional Supplements Benefit Patients With Nonalcoholic Steatohepatitis and Nonalcoholic Fatty Liver Disease?” Cureus, vol. 15, no. 6, June 2023, p. e40849. pmc.ncbi.nlm.nih.gov, https://doi.org/10.7759/cureus.40849.
